CREATINE
Creatine monohydrate is a popular supplement that has been used for decades to enhance physical performance. From athletes to fitness enthusiasts, many people have turned to creatine monohydrate to help them achieve their muscle gain, endurance, strength, and performance goals.
This supplement has been extensively researched and has been shown to have numerous benefits in these areas. In this article, we will explore the evidence supporting the use of creatine monohydrate for enhancing physical performance, as well as potential risks and side effects. We will also discuss how to properly take creatine monohydrate to maximize its benefits.
Overall, we aim to provide a comprehensive overview of the benefits and drawbacks of creatine monohydrate supplementation, allowing individuals to make an informed decision about whether this supplement is right for them.
Table of Contents
- What is creatine?
- Formulations & Variants
- Loading
- What Are The Main Benefits?
- Can Creatine Increase Your Testosterone Levels?
- What Are Creatine’s Main Drawbacks?
- Is Creatine Safe For Your Kidneys?
- Does Creatine Cause Hair Loss?
- How Does Creatine Work?
- Cellular Hydration
- Cytoprotection
- Neurogenesis
- Glycogen
- Power Output
- Resistance Exercise
- Muscle Growth & Hypertrophy
- Nutrient Timing & Dosing
- Sprinting
- Injury & Rehabilitation
- Bone Mass
- Summary
What is creatine?
Creatine is a molecule that is produced in the body from amino acids. Specifically, creatine is composed of L-arginine, glycine and methionine.
It’s primarily made in the liver and (to a lesser extent) in the kidneys and pancreas. [1]
Creatine can also be found in some animal-based foods and is most prevalent in meat and fish. [1]
Some (uncooked) meats have high levels of creatine:
- Beef, with minimal visible connective tissue: 5 g per 1.1 kg or 2.15-2.5 g/lb (4.74-5.51 g/kg).
- Chicken: 3.4 g/kg
- Rabbit: 3.4 g/kg
- Cardiac tissue (ox): 2.5 g/kg
- Cardiac tissue (pig): 1.5 g/kg
Some (uncooked) meats have low levels of creatine:
Other compounds containing creatine include:
According to the NHANES III survey, the average daily consumption of creatine from food sources among Americans (19-39 years old) is about 7.9 mmol (1.08g) for men and 5 mmol (0.64g) for women. This is below the “2g/day consumed via the diet” estimate that many studies reference.
Main Takeaway: Creatine accumulates in the same organs in meat products as in humans. Tissues with a high creatine content include the heart and the skeletal muscles. Dairy products have minimal creatine content and meat is the only significant source of dietary creatine.
Creatine from food is digested slower than creatine taken as a supplement, but total bioavailability is identical.
Creatine plays an important role in energy metabolism, particularly in high-intensity exercise. Creatine stores high-energy phosphate groups in the form of phosphocreatine. These phosphate groups are donated to ADP to regenerate it to ATP, the primary energy carrier in the body.
When creatine is taken in supplement form, it is typically in the form of creatine monohydrate. This is the most well-studied and widely-used form of creatine supplementation.
There are other forms of creatine supplementation available, including creatine ethyl ester, creatine hydrochloride, and buffered creatine. These forms of creatine are marketed as being more easily absorbed by the body or causing fewer side effects. However, there is little scientific evidence to support the use of these forms of creatine over creatine monohydrate, which has been extensively studied and shown to be safe and effective.
Formulations & Variants
The most common form of creatine is creatine monohydrate and if not otherwise mentioned, is the default form of creatine used in most studies on creatine. It has fairly decent intestinal absorption. [1]
This basic form of creatine comes in two forms, one of which involves the removal of the monohydrate (creatine anhydrous) that converts to creatine monohydrate in an aqueous environment, but due to the exclusion of the monohydrate it is 100% creatine by weight despite creatine monohydrate being 88% creatine by weight, as the monohydrate is 12%. This allows more creatine to be present in a concentrated formula, like capsules.
Creatine monohydrate can also be micronized (commonly sold as “Micronized Creatine”) which is a mechanical process to reduce particulate size and increase the water solubility of creatine. In regard to supplementation, it is equivalent to creatine monohydrate.
Main Takeaway: Creatine is most commonly found in the basic form of creatine monohydrate, which is the standard form and usually recommended due to the low price. It can also be micronized to improve water solubility, or the monohydrate can be temporarily removed to concentrate creatine in a small volume supplement. Neither alteration changes the properties of creatine.
Creatine hydrochloride (Creatine HCl) is a form of creatine characterized by the molecule being bound to a hydrochloric acid moiety. It is claimed to require a lower dosage than creatine monohydrate, but this claim has not been tested. Creatine hydrochloride likely forms into free creatine and free hydrochloric acid in the aqueous environment of the stomach, which would mean it is approximately bioequivalent to creatine monohydrate.
Main Takeaway: Creatine HCl is touted to require a lower dosage, but this has not been proven through studies and seems unlikely, since the stomach has an abundance of HCl anyway and creatine will freely dissociate with HCl in the stomach. Thus, both creatine HCl and creatine monohydrate form free creatine in the stomach.
Liquid creatine is ineffective as a creatine supplement due to its limited stability in solution. This shouldn’t be an issue for people preparing a creatine solution at home, since it takes a few days to for creatine to degrade. This is a problem for the manufacturers, where creatine in solution has a limited shelf-life.
Liquid creatine has been shown to be less effective than creatine monohydrate due to the passive breakdown of creatine into creatinine over a period of days, which occurs when it is suspended in solution.
This breakdown is not an issue for at-home use when creatine is added to shakes, but it is a concern from a manufacturing perspective in regard to shelf-life before use.
Buffered creatine (Kre-Alkylyn is the brand name) is touted to enhance the effects of creatine monohydrate due to a higher pH level, which enables better translocation across the cytoplasmic membrane and more accumulation in muscle tissues.
Buffered creatine against basic creatine monohydrate has no significant differences in regard to the effects or the accumulation of creatine in muscle tissue as well as no significant differences in the amount of adverse side-effects.
Main Takeaway: “Buffered” creatine (Kre-Alkylyn) is suggested to be a better absorbed form of creatine supplementation, but it can be rapidly neutralized in the stomach if it is not in an enteric coating. Even if it is enteric coated, there is no evidence to support its efficacy above creatine monohydrate.
Creatine ethyl-ester increases muscle levels of creatine to a lesser degree than creatine monohydrate. It may also result in higher serum creatinine levels due to creatine ethyl ester being converted into creatinine via non-enzymatic means in an environment similar to the digestive tract. [1]
Creatine ethyl-ester is more a pronutrient for creatinine rather than creatine, and was originally created in an attempt to bypass the creatine transporter.
At equal doses to creatine monohydrate, ethyl ester has failed to increase water weight after 28 days of administration (indicative of muscle deposition rates of creatine, which are seemingly absent with ethyl-ester). Direct studies on creatine ethyl-ester show it to be less effective than creatine monohydrate, on par with a placebo.
Main Takeaway: Creatine ethyl-ester is likely ineffective as a creatine supplement for general use.
Magnesium-chelated creatine typically exerts the same ergogenic effects as creatine monohydrate at low doses. It was created because carbohydrates tend to beneficially influence creatine metabolism and magnesium is also implicated in carbohydrate metabolism and creatine metabolism. [1]
Magnesium chelated creatine may be useful for increasing muscle strength output with a similar potency to creatine monohydrate, but without the water weight gain, as there are noted differences, but they are statistically insignificant. [1]
Main Takeaway: Creatine magnesium chelate has some limited evidence for it being more effective than creatine monohydrate, but this has not been investigated further.
Creatine nitrate in which a nitrate (NO3) is bound to the creatine molecule doesn’t appear to enhance athletic performance more than monohydrate.
Other variants of creatine with increased water solubility such as creatine citrate and creatine malate don’t differ greatly from monohydrate in regard to absorption or kinetics.
Creatine pyruvate in an isomolar dose relative to creatine monohydrate has been shown to produce higher plasma levels of creatine (peak and AUC) with no discernible differences in absorption or excretion values. The same study noted increased performance from creatine pyruvate at low (4.4g creatine equivalence) doses relative to citrate and monohydrate, possibly due to the pyruvate group.
Creatine α-ketoglutarate has little research done on it and has been experimentally unproven.
Polyethylene glycosylated creatine seems to be as effective as creatine monohydrate at a lower dose (1.25-2.5g relative to 5g monohydrate), but does not seem to be comparable in all aspects. [1]
Creatine gluconate is a form of creatine supplementation in which the creatine molecule is bound to a glucose molecule and it is thought to be better absorbed when taken alongside food, since many other gluconate molecules, particular in the context of minerals like magnesium, are absorbed better with food. It currently does not have any studies conducted on it.
Cyclocreatine is a synthetic analogue of creatine in a cyclic form. It appears to be passively diffused through membranes and not subject to the creatine transporter, which can be beneficial for cases where creatine transporter function is compromised (creatine non-response and SLG6A8 deficiency). Similar to other forms of creatine, it buffers ATP concentrations, although its efficacy as a supplement in otherwise healthy people is currently unknown.
Main Takeaway: Stick to the proven and extremely affordable creatine monohydrate.
Loading
Creatine retention (assessed by urinary analysis) tends to be very high on the first loading dose and declines throughout the loading phase. This is likely due to increased muscular uptake when creatine stores are relatively low, which has been noted in vegetarians. So, creatine absorption is very high initially, but decreases througout the loading phase, as muscle creatine stores increase.
Coingestion of creatine with carbohydrate is known to increase glycogen accrual in skeletal muscle (possibly resulting in increased cell volume) although the creatine content in muscles does not appear to be significantly increased.
Loading Protocol:
- Take 5grams of creatine monohydrate 4-5 times per day for the first 5 days
- Continue with 3-5grams indefinitely, preferably before or after your workout or with a meal if it’s a non training day to avoid feeling nauseus.
This will ensure that you get all the benefits within a week of intake.
What Are The Main Benefits?
One of the most significant benefits of creatine supplementation is its ability to improve strength and power output during resistance exercise. There is a substantial body of research supporting this use of creatine, and the effects can be quite remarkable for a dietary supplement. Moreover, when combined with resistance training, creatine may slightly increase lean muscle mass. There have also been several studies investigating the effects of creatine on anaerobic running capacity, and while the findings are somewhat inconsistent, the general consensus is that creatine may lead to a minor improvement in performance.
While the research on the effects of creatine on cognitive performance is not as extensive as it is for physical performance, there is evidence to suggest that creatine supplementation may be beneficial in certain situations.
Creatine appears to reduce mental fatigue in scenarios such as demanding mental activity and sleep deprivation. [1]
Creatine may also improve working memory, though likely only for people with below-average creatine levels, such as vegetarians and older adults. [1]
Can Creatine Increase Your Testosterone Levels?
Creatine is known for reliably improving physical performance.
While creatine has been marketed as a testosterone booster, there is limited evidence to support this claim. Dietary supplements are often tested for their effects on hormones, especially if they have anabolic properties, as creatine does. Creatine works by increasing the amount of adenosine triphosphate (ATP) available to your muscles, which can help you exercise more intensely and lift heavier weights, ultimately leading to greater muscle growth.
However, the anabolic effect of creatine is indirect and mediated by increased workout intensity.
It is well-established that weightlifting triggers a temporary boost in testosterone production. [1]
Since creatine enables you to lift heavier weights during exercise, it had been suggested that supplementing with creatine may lead to an increase in testosterone levels following a workout.
The evidence for this however, is scarce. The notion that creatine may increase testosterone levels is supported by reference to three randomized controlled trials (RCTs).
The first study randomized 20 healthy young rugby players into two groups.
The creatine group was given a loading dose of 25 g/day for one week, followed by a maintenance dose of 5 g/day for two weeks. Surprisingly, the participants’ testosterone levels did not change significantly in either the placebo group or the creatine group. However, at the end of the study, the creatine group showed a significant 0.12 ng/mL (12 ng/dL) increase in dihydrotestosterone (DHT), a highly active androgen that is converted from testosterone and is known to contribute to hair loss. Notably, this is the only RCT to date that has investigated the effects of creatine on DHT.
Both the second and third RCTs randomized 20 healthy, active young men into two groups each. The creatine group in both studies was given a dose of 20 g/day for one week. In both studies, the creatine group saw a significant increase in testosterone levels, whereas the placebo group saw no change. The first study reported a 0.57 ng/mL (57 ng/dL) increase in testosterone, while the second study found an increase of 1.5 ng/mL (150 ng/dL).
The hormonal increases observed in all three studies were statistically significant, but they were relatively small and did not push the participants outside of normal hormonal ranges. These three studies are frequently referenced as evidence that creatine supplementation may lead to an increase in testosterone levels.
In addition to the three RCTs previously discussed, ten other RCTs involving a total of 218 participants have also examined the relationship between creatine supplementation and testosterone levels. These studies ranged in duration from 6 days to 10 weeks and employed daily creatine doses that varied from 3 to 25 g, with one study administering 4 pre-workout doses over a period of 10 weeks.
All ten of these RCTs found that there was no significant impact of creatine supplementation on testosterone levels. [1, 2, 3, 4, 5, 6, 7, 8, 9]
This is in contrast to the three studies previously mentioned that reported small but significant increases in testosterone levels following creatine supplementation. The preponderance of evidence from the majority of studies suggests that there is no significant relationship between creatine and testosterone, indicating that the hormonal effects of creatine may be limited and may not apply to all populations.
Of the ten RCTs that found no significant impact of creatine supplementation on testosterone levels, nine used creatine monohydrate, which is the most commonly used form of creatine. The remaining study used creatine malate at a dosage of 0.07 g per kilogram of body weight per day and was conducted over a period of six weeks with 19 young male runners.
All but two of the RCTs were in active, healthy young males (one in untrained young males, another in trained older males).
When evaluating the effects of creatine on testosterone levels, it is important to consider not only the number but also the length of the studies. The studies that observed an increase in testosterone [1] or DHT with creatine supplementation lasted between 1 and 3 weeks, while those that did not observe an increase lasted up to 12 weeks. [1, 2, 3, 4, 5, 6, 7, 8, 9, 10]
While longer studies are not necessarily more reliable than short ones, they may be more relevant in real-world settings. For instance, an increase in testosterone levels may have a greater impact on muscle mass over several months than over just a few days.
No studies have been conducted to investigate the effects of creatine supplementation on testosterone levels in men with low testosterone. Additionally, there are no studies on the effects of creatine supplementation on female testosterone levels. However, based on the largely negative results from the male studies, it is reasonable to suggest that creatine supplementation does not affect female testosterone levels.
Main Takeaway: Creatine supplementation enhances exercise performance, but most studies show that it has no effect on testosterone levels.
What Are Creatine’s Main Drawbacks?
When too much creatine is consumed at one time, it can cause diarrhea and nausea. In order to prevent this, it is recommended to spread the doses throughout the day and take them with meals. Creatine supplementation is known to cause weight gain, which can be attributed to an increase in total body water.
Is Creatine Safe For Your Kidneys?
Creatine that is ingested or produced by the liver is stored in various tissues of the body, including skeletal muscles and the brain.
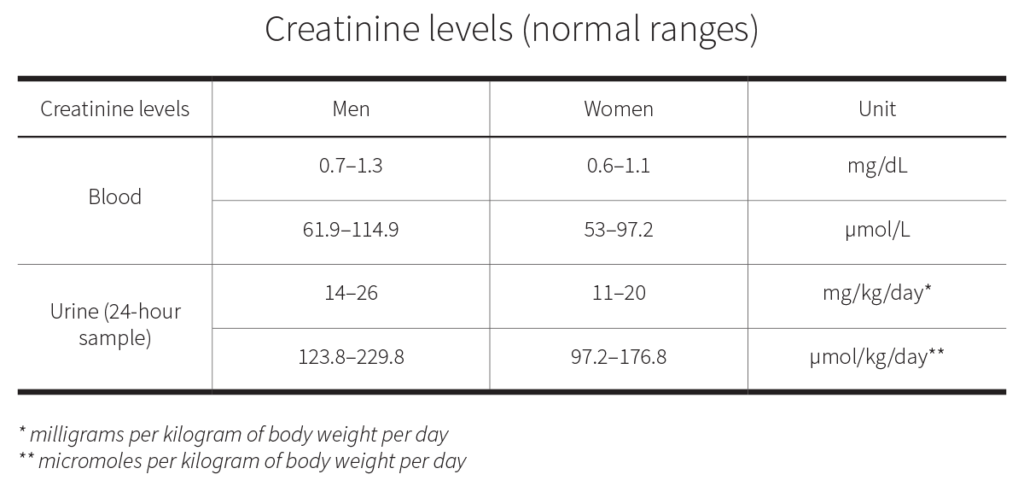
These tissues convert creatine into phosphocreatine, which is used to recycle adenosine triphosphate (ATP) during energy production. A byproduct of this process is creatinine, which is eliminated from the body by the kidneys. When the kidneys function properly, they excrete creatinine without changes. However, if kidney function decreases, then so does the clearance of creatinine. Creatinine clearance can be estimated from a blood test or measured through a combination of blood test and 24-hour urine sample. High levels of creatinine in the blood can be an indicator of reduced kidney function.
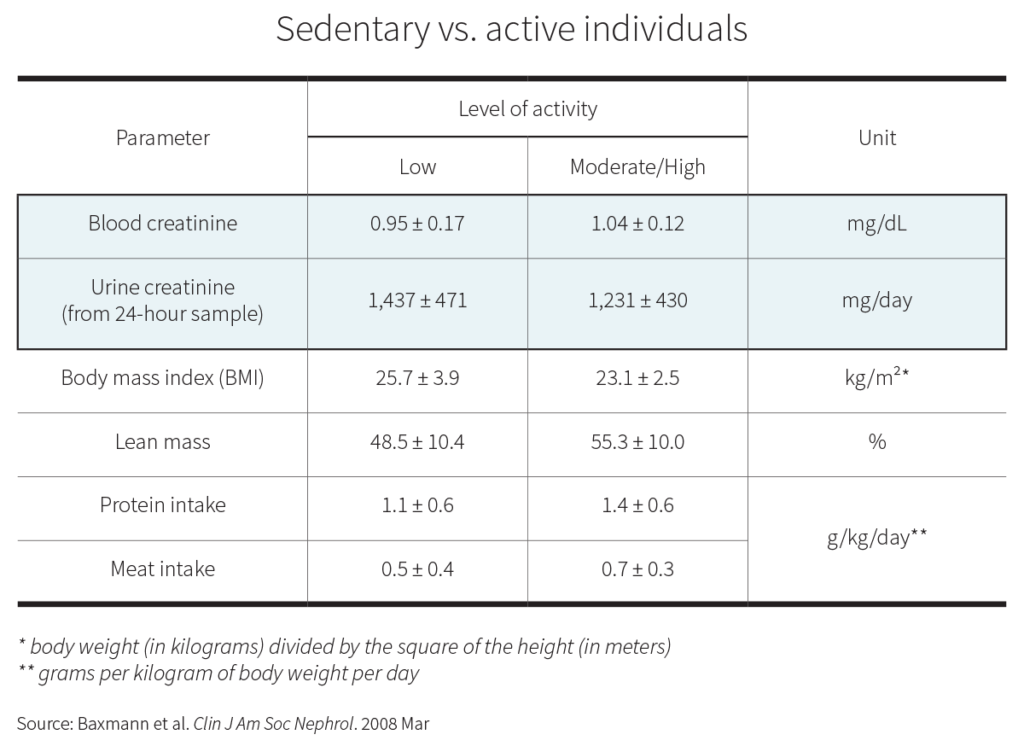
The vast majority of your body’s creatine stores are located in your skeletal muscles, accounting for >90%. This means that the more muscle you have and the more you use it, the more creatinine your body will produce. [1]
Greater animal protein intake has been associated with greater muscle mass [1] and higher creatinine excretion.
While supplemental creatine can increase your blood levels of creatinine beyond the normal ranges [1] does that mean that your kidneys are being damaged?
Scientific reviews examining both the short- and long-term safety of supplemental creatine have consistently found no evidence of adverse effects on kidney function. [1, 2, 3, 4, 5, 6, 7]
Most healthy people can benefit from creatine supplementation with a daily dose of 3-5 grams. However, creatine nonresponders or people with high muscle mass may benefit from a higher dose of up to 10 grams per day.
Doses >10 g/day have been found not to impair kidney function, but there are fewer long-term trials on such high doses.
In healthy adults, doses ≤5 g/day are unlikely to increase creatinine levels significantly, [1, 2] but higher doses might cause a false positive — an increase in creatinine that may be misinterpreted as a sign of kidney damage. [1, 2]
Most studies, however, have noted only a small increase in creatinine levels even with doses ≈20 g/day. [1, 2]
Although taking creatine may increase creatinine levels, long- and short-term studies have found that creatine doses ≤10g/day don’t impair kidney health in people with healthy kidneys.
In people whose kidneys don’t function optimally, supplemental creatine seems to be safe, too. One case study found that a man’s single kidney suffered no harm from 20 g/day for 5 days followed by 5 g/day for 30 days. An RCT in type 2 diabetics with various stages of kidney disease showed no significant decline in kidney function from 5 g/day for 12 weeks. Two clinical trials saw no detriment in people with kidney disease. [1]
Limited short-term evidence indicates that people with suboptimal kidney function may safely supplement with creatine. However, long-term studies are lacking.
If you are someone with kidney dysfunction, or at risk for developing kidney dysfunction, you might wish to forgo creatine, or otherwise take only the lowest effective dose (3 g/day). Since creatine can increase water retention, it could theoretically harm people whose kidney disorder is being treated with diuretics, which cause water loss.
Does Creatine Cause Hair Loss?
A 2009 study implicated that creatine supplementation might worsen hair loss. In this RCT, males given creatine experienced a significant increase in their blood levels of dihydrotestosterone (DHT) — an androgen that contributes to hair loss, particularly in males. By interacting with hair follicles, DHT can induce hair loss. [1]
The likelihood of a hair falling out, whether due to DHT sensitivity or other factors, depends on a variety of factors, including its location on the scalp. For example, in male-pattern hair loss, hair thinning typically occurs first at the crown and hairline. Additionally, genetic factors also play a significant role in determining hair loss susceptibility. [1]
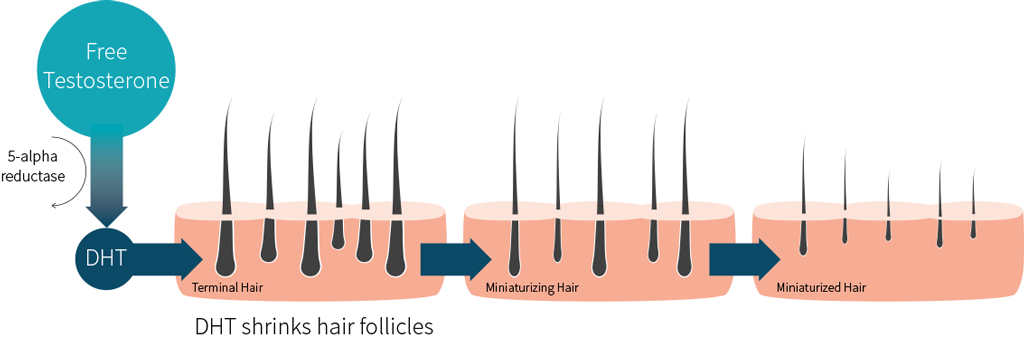
DHT is a metabolite of another androgen: testosterone. The enzyme 5-alpha-reductase converts free testosterone (testosterone not bound to either serum albumin or sex hormone binding globulin (SHBG)) to DHT. DHT can bind to receptors on the hair follicles of the scalp, causing them to shrink and cease hair production over time. [1]
While male-pattern hair loss is a well-documented and studied phenomenon, female-pattern hair loss is less well understood.
While genetic factors also do contribute to female-pattern hair-loss, the importance played by the genes identified in females is less clear than the importance played by the genes identified in males. Similarly, DHT is thought to play a lesser role in female hair loss. Additional factors, such as estrogen levels, are thought to have some influence on female hair loss, but there is conflicting evidence.
Like mentioned earlier, only one RCT has linked creatine supplementation with an increase in DHT. This study was done in 20 healthy young male rugby players, randomized into two groups: one group took a placebo, while the other supplemented with creatine monohydrate by taking a loading dose (25 g/day) for 7 days, then a maintenance dose (5 g/day) for 14 days.
Changes in testosterone were not significantly different between the two groups, but DHT was significantly increased at day 7 (by 0.44 ng/mL above baseline, so 56.1%) and day 21 (by 0.12 ng/mL above baseline, so 40.8%) in the creatine group.
A published response to this study inquired mostly about methods but found no statistical faults his study tested its creatine for 25 different potential adulterants, such as stimulants and androgenic steroids. None were detected, ruling out the possibility that changes in DHT were due to illegal contaminants.
This has been the only RCT testing creatine’s effects on DHT. As mentioned previously, only two RCTs saw a significant increase in testosterone when supplementing with 20 g of creatine per day over 6 days and 7 days. Ten RCTs have found no effect of creatine on testosterone. Importantly, five of these RCTs specifically tested creatine’s effects on _free_ testosterone, the form that gets converted into DHT. All saw no significant increases.
Creatine might non-significantly increase free testosterone yet significantly increase DHT (i.e., a small increase in free testosterone, the base material of DHT, could lead to a much greater increase in DHT). Second, creatine might be upregulating 5-alpha-reductase, the enzyme that converts free testosterone to DHT. The current evidence is not strong enough to conclusively support any particular theory.
Main Takeaway: There is limited evidence on the link between creatine and DHT, and no studies have directly examined the effect of creatine on hair loss.
While one study in males found a potential link between creatine and increased DHT, other studies have not found a significant effect of creatine on testosterone levels.
It is also important to note that hair loss is a complex issue influenced by multiple factors, and an increase in DHT levels does not necessarily mean that hair loss will occur. Further research is needed to better understand the potential relationship between creatine, DHT, and hair loss.
How Does Creatine Work?
Carbohydrates provide quick energy in an anaerobic environment (high-intensity exercise), while fats provide sustained energy during periods of high oxygen availability (low-intensity exercise or rest).
The energy from the breakdown of carbohydrates, fats, and ketones is stored in adenosine triphosphate (ATP), which in turn powers most cellular processes. When cells use ATP for energy, this molecule is converted into adenosine diphosphate (ADP) and adenosine monophosphate (AMP). Creatine exists in cells to donate a phosphate group (energy) to ADP, turning this molecule back into ATP. [1, 2, 3]
By increasing the overall pool of cellular phosphocreatine, creatine supplementation can accelerate the reycling of ADP into ATP, making more energy available for high-intensity exercise. Since ATP stores are rapidly depleted during intense muscular effort, one of the major benefits of creatine supplementation is its ability to regenerate ATP stores faster, which can promote increased strength and power output.
Over 95% of creatine is stored in muscle at a maximum cellular concentration of 30uM. Creatine storage capacity is limited, though it increases as muscle mass increases.
A 70 kg male with an average physique is assumed to have total creatine stores of approximately 120g.
The body can store a lot more energy as glycogen in the liver, brain, and muscles, [1] and even more as fat.
Main Takeaway: Creatine is a peptide that acts as an energy substrate by storing high-energy phosphate groups that can help regenerate ATP, the main source of cellular energy.
When creatine intake increases, either through food or supplementation, cellular energy stores also increase, which facilitates the short-term regeneration of ATP. However, these stores have their limits, and glucose or fatty acids take over to replenish ATP over longer periods.
The liver is the primary site of endogenous creatine synthesis, with additional contributions from the kidneys and pancreas. The synthesis process involves the enzyme Arginine:Glycine amidinotransferase (AGAT) catalyzing the combination of glycine and arginine to form ornithine and guanidoacetate, which is the first step in creatine synthesis. In cases of deficiency in this enzyme, which is rare, mild mental retardation and muscular weakness can occur.
AGAT is also the primary regulatory step, and an excess of dietary creatine can suppress activity of AGAT to reduce creatine synthesis by reducing AGAT mRNA levels, rather than resulting in competitive inhibition.
After AGAT forms guanidoacetate, guanidoacetate then receives a methyl donation from S-adenosyl methionine via GAMT to produce creatine, with S-adenosylhomocysteine formed as a byproduct. Deficiencies in GAMT are rarer but more severe, resulting in symptoms such as severe mental retardation and autism-like behavior.
For the most part, the above reactions occur in the liver, where most systemic creatine is synthesized. Neurons also possess the capability to synthesize their own creatine.
Main Takeaway: Creatine is synthesized through the combination of glycine and arginine, which forms guanidoacetate that is then methylated to produce creatine. Any issues with the process of creatine synthesis can lead to muscle disorders and mental retardation.
Cellular Hydration
Upon absorption, creatine can cause cells to increase in volume by drawing in water. This process, known as “cell volumization,” is thought to promote an anabolic state in cells which can decrease protein breakdown and increase DNA synthesis. [1, 2]
An increase in cellular viability assessed via phase angle (measuring body cell mass) has been noted in humans during supplementation of creatine.
Glycogen synthesis is known to respond directly and positively to cellular swelling. Stress proteins of the MAPK class (p38 and JNK) as well as heat shock protein 27 (Hsp27) are activated in response to increasing osmolarity. [1]
Activation of MAPK signaling in skeletal muscle cells is known to induce myocyte differentiation via GSK3β and MEF2 signaling, which can induce muscle cell growth. [1]
Main Takeaway: Cellular swelling, which occurs when creatine is absorbed and pulls water into cells, is associated with increased muscle cell growth. This is due to the activation of stress response proteins, specifically those in the MAPK class, which in turn promotes muscle protein synthesis. These mechanisms do not rely on the creatine kinase cycle.
It has been observed that inducing hypertonicity, which refers to a reduction in cellular swelling, can increase the mRNA of the creatine transporter. This is believed to occur as a result of increased cellular creatine uptake aimed at normalizing creatine levels. This has been noted in both muscle cells and endothelial cells, but is thought to apply to all cells.
The way in which the body regulates creatine uptake is similar to that of other osmolytic agents like myo-inositol or taurine. During periods of hypertonicity, the uptake of these agents is increased to promote cellular swelling. This response may be attributed to the normalization of creatine levels in the cell.
Main Takeaway: The expression of the creatine transporter and thus the cellular uptake of creatine is modulated by the cellular hydration status. This regulatory mechanism is similar to that observed for other osmolytes in the human body.
Cytoprotection
Phosphocreatine, the higher energy form of creatine, can associate with and protect cell membranes.
This was first observed in Drosophilia, which do not express the creatine kinase enzyme (and cannot use creatine for energy purposes) yet still received cellular protection from creatine.
Neuroprotection
Creatine, through its ability to act as an energy reserve, attenuates neuron death induced by the MPTP toxin that can produce Parkinson’s disease-like effects in research animals, reduces glutamate-induced excitotoxicity, attenuates rotenone-induced toxicity, L-DOPA induced dyskinesia, 3-nitropropinoic acid, and preserves growth rate of neurons during exposure to corticosteroids (like cortisol), which can reduce neuron growth rates.
These effects are secondary to creatine being a source of phosphate groups and acting as an energy reserve. The longer a cell has energy, the longer it can preserve the integrity of the cell membrane by preserving integrity of the Na+/K+-ATPase and Ca2+-ATPase enzymes. [1, 2]
Preserving ATP allows creatine to act via a nongenomic response (not requiring the nuclear DNA to transcribe anything), and appears to work secondary to MAPK and PI3K pathways.
Main Takeaway: A protective effect on neurons by creatine, secondary to its ability to donate phosphate groups, exists and appears to be quite general in its protective effects.
Neurogenesis
The concentration of creatine that increases mitochondrial respiration in skeletal muscle is 20mM. This concentration also appears to work similarly in hippocampal cells. This promotes endogenous PSD-95 clusters and subsequently synaptic neurogenesis (thought to simply be secondary to promoting mitochondrial function).
Main Takeaway: Mitochondrial function appears to promote neuronal growth and proliferation, and at least in vitro, creatine is known to do the same and promote growth.
Glycogen
Creatine is known to increase skeletal muscle cellular volume alongside increases in water weight gain. Since glycogen itself also increases the osmolytic balance of a cell (draws in water) [1] and preliminary evidence shows a strong trend of creatine augmenting glycogen loading, creatine is thought to be related to an increase in cell volume, which is known to promote glycogen synthesis.
Main Takeaway: There appears to be a positive correlation between creatine and glycogen levels in muscle cells, such that an increase in one is often accompanied by an increase in the other. As a result, it is believed that creatine supplementation may contribute to glycogen replenishment and loading.
Creatine has been found to increase skeletal muscle glycogen when given to sedentary adults for a loading and maintenance phase for 37 days at 2g (13.5% after five days of loading, but returning to baseline at the end of the trial). Exercise was not enforced in this study and despite a normalization of glycogen after the trial, total creatine and ATP was still higher than placebo.
A loading protocol appears to have failed elsewhere in increasing glycogen stores in sedentary people subject to an aerobic exercise test before and after the loading phase.
A study conducted on individuals who underwent glycogen depletion through exercise found that the control group, who followed an exercise and glycogen-replenishing diet, experienced a 41% increase in glycogen levels. However, when creatine loading was introduced, the glycogen increase in the experimental group rose to 53%.
When creatine was used to enhance the accumulation of glycogen in the muscle, combining it with carbohydrate intake did not result in further increase in creatine loading in the muscle, compared to the control group. Taking creatine supplements after exercising led to a 37% increase in intramuscular creatine levels in the non-exercised leg and a 46% increase in the exercised leg.
Main Takeaway: When determining how glycogen is influenced under supplementation of creatine, taking creatine supplements along with carbohydrates can enhance the synthesis and accumulation of glycogen in skeletal muscles. However, while creatine supplementation can speed up glycogen replenishment rates, it does not seem to result in an increase in the amount of creatine that enters the cell.
Power Output
Two meta-analytical studies conducted on the subject have shown that supplementation of creatine leads to a notable increase in power in both males and females when taken for up to 8 weeks. The results indicate that the improvement over placebo is sustained during this period, without any further significant enhancements. [1]
Research suggests that resistance training regimens lead to significantly higher rates of power output, up to 78.5% more, when supplemented with creatine, compared to a placebo. Specifically, in active trained men with no prior creatine experience, this effect is estimated to translate to a 7kg increase in the bench press and a 10kg increase in the squat over an 8-week period.
Resistance Exercise
Resistance exercise enhances the rate of creatine uptake into muscle cells that are actively engaged. Initially thought to be a byproduct of enhanced blood flow, the enhanced creatine uptake is now thought to be due to allosteric modifications of the creatine transporter, which enhances its maximal capacity.
Muscle Growth & Hypertrophy
Supplementing with creatine has been found to increase the size of muscle fibers, irrespective of protein synthesis. This is due to the fact that the intake of creatine leads to an increase in water content within muscle cells, which in turn increases their diameter. In a study where 20g of creatine was ingested alongside dextrose at a ratio of 1:7.5, the diameter of type I, IIa, and IIx muscle fibers increased by 9%, 5%, and 4%, respectively.
This cellular influx may also decrease protein oxidation rates, which leads to increases in nitrogen balance and indirectly increases muscle mass. This lowering of protein oxidation is from signaling changes caused vicariously through cell swelling [1] and appears to upregulate 216 genes in a range of 1.3 to 5-fold increases, with the largest increase seen in the protein involved in satellite cell recruitment, sphingosine kinase-1.
Most importantly for muscle hypertrophy, the protein content of PKBa/Akt1, p38 MAPK, and ERK6 increased 2.8+/-1.2 fold.
Nutrient Timing & Dosing
Research has demonstrated that taking 12g of creatine over a two-week period before undergoing an endurance running test (at 65-70% VO2 max for one hour) can help reduce the increase in lactate levels and the tryptophan/BCAA ratio. Additionally, this supplementation was found to reduce the increase in serum protein catabolites, indicating an anti-catabolic effect.
In otherwise healthy bodybuilders, supplementation of creatine at 5g either immediately before or after a weight training session (with no directive on non training days) over the course of four weeks noted that while both groups improved, there was no significant difference between groups overall.
The same result was found in another study with 0.1g/kg creatine thrice weekly over 12 weeks in otherwise healthy adults.
In contrast to the above null effects, ingestion of creatine both before and after a workout (alongside protein and carbohydrate) over 10 weeks seems to promote muscle growth more than the same supplement taken in the morning, farther away from the time of the workout.
The benefits of creatine around the workout, relative to other times, have been hypothesized to be related to an upregulation of creatine transport secondary to muscle contraction, a known phenomena.
Main Takeaway: The lowest dose of creatine sufficient to increase muscular creatine stores in otherwise healthy but sedentary people (2 grams) appears to be insufficient for athletes. The benefits of creatine supplementation appear to be more prominent when taken closer to the resistance training workout than when compared to supplementation at other times of the day. This benefit applies equally to taking creatine before the workout and/or after the workout.
Heat Tolerance
Higher percieved effort during heat (or due to elevations in body heat) are thought to be mediated by either the serotonergic system (suppresses performance) or the dopaminergic system (enhances performance), [1] and creatine is thought to be involved in percieved effort during heat training since it has been noted previously to interact with neurotransmission by enhancing both serotonergic and dopaminergic neurotransmission.
When exercising in heat, supplemental creatine (loading phase with carbohydrates) appears to be able to reduce symptoms of hyperthermia, such as perceived physical exertion. Despite physical performance enhancement only occurring in responders, the benefits of heat tolerance occurred in both groups of people.
Endurance exercise is also known to produce heat from skeletal muscle tissue, and an increase in internal temperature occurs when the production of heat (from metabolism) exceeds release. This increase in heat is accelerated when training in hot environments and it is thought to be beneficial to retain water (hydration) during exercise, since more water allows a preservation of plasma volume (PV) and the sweat response reduces internal temperature. [1]
This particular phenomena may only apply to endurance exercise, since creatine is able to increase sprint performance in heat, independent of altering the decline in PV and sweat rates.
Sprinting
The recovery period between sprint sets is known to be associated with phosphocreatine regeneration and this resynthesis rate is highly associated with actual physical performance during the sprints.
Creatine supplementation at 300mg/kg for one week (loading with no maintenance) in youth subject to six repeated 35m sprints (10s rest) noted that the increased average and peak power output seen in creatine was not met with a reduction in fatigue, although there was an attenuation in inflammation from exercise (TNFα and CRP).
Creatine supplementation appears to be effective at increasing power output in anaerobic cardiovascular exercise, [1, 2, 3] and has been implicated in increasing the lactate threshold as well as time to volitional fatigue within 6 days after stating supplementation (20g daily, divided into 4 doses with 15g glucose).
Some studies note no significant benefit [1] although at least one author has suggested this may be due to calculation errors. Regardless, there is still some counter evidence that is not subject to said calculation errors that suggests no statistically significant benefit.
Main Takeaway: When examining repeated sprinting tests (sprint, rest a minute or less, repeat) the rate of phosphocreatine resynthesis appears to be a positive influence on performance and supplemental creatine appears to be beneficial.
Injury & Rehabilitation
Bone Mass
Animal evidence at this moment shows promise for creatine’s effects on bone mass, [1]
but a study in spontaneously hypertensive rats failed to find any benefits for unknown reasons.
Safety & Toxicology
There are no clinically significant side effects of acute creatine supplementation. Numerous trials have been conducted in humans with varying dosages, and the side effects have been limited to gastrointestinal distress (from too much creatine consumption at once) and cramping (from insufficient hydration). [1, 2]
A dose of 5g daily has strong evidence supporting it not causing any adverse side effects and 10g has been used daily for 310 days in older adults (aged 57+/-11.1) with no significant differences from placebo.
Such a dose has also been demonstrated for long-term safety for people with Parkinson’s disease, and at least one small retrospective study in athletes (surverying people taking creatine for up to or over a year) failed to find any significant differences in a battery of serum health parameters. Other studies measuring serum parameters have also failed to find abnormalities outside the normal range.
Studies that use a dosage range typical of creatine supplementation (in the range of 5g a day following an acute loading period) note increases to total body water of 6.2% (3.74lbs) over 9 weeks and 1.1kg over 42 days.
Some studies comparing creatine paired with training against training itself fail to find a significant difference in percentage of water gained (which is inherently to activity) with standard oral doses of creatine [1, 2] despite more overall water weight being gained, due to an equal gain of dry mass in muscles.
Low dose creatine supplementation of 0.03g/kg or 2.3g daily doesn’t appear to increase water retention. One study has quantified the percentage increase in mass of muscle cells to be 55% water, suggesting the two groups are fairly equal.
In regard to the loading period, two reviews suggest that the range of weight gain associated with creatine supplementation at 20g for 7 days is in the range of 0.9-1.8kg (1.98-3.96lbs). [1] The highest reported increase in water weight associated with creatine loading, although measured a month after loading started (after a maintenance phase) was 3.8kg (8.36lbs).
Creatine does not tend to disturb the ratios of water to dry mass in various tissues measured.
Summary
Tldr; Creatine is a molecule that is produced in the body from amino acids. Specifically, creatine is composed of L-arginine, glycine and methionine.
It’s primarily made in the liver and (to a lesser extent) in the kidneys and pancreas. It is found in high levels in the skeletal muscles and the heart, but also to some degree in almost every cell of all vertebrates and various invertebrates.
Dairy products have minimal creatine content and meat is the only significant source of dietary creatine.
The average daily consumption of creatine from food sources among Americans (19-39 years old) is about 1.08g for men and 0.64g for women. This is below the “2g/day consumed via the diet” estimate that many studies reference, negating the importance of supplementation.
When creatine intake increases, either through food or supplementation, cellular energy stores also increase, which facilitates the short-term regeneration of ATP. However, these stores have their limits, and glucose or fatty acids take over to replenish ATP over longer periods.
When creatine is taken in supplement form, it is typically in the form of creatine monohydrate. This is the most well-studied and widely-used form of creatine supplementation, and usually recommended due to the low price. It can also be micronized to improve water solubility, or the monohydrate can be temporarily removed to concentrate creatine in a small volume supplement. Neither alteration changes the properties of creatine. Creatine from food is digested slower than creatine taken as a supplement, but total bioavailability is identical.
Creatine HCl is touted to require a lower dosage, but this has not been proven through studies and seems unlikely, since the stomach has an abundance of HCl anyway and creatine will freely dissociate with HCl in the stomach. Thus, both creatine HCl and creatine monohydrate form free creatine in the stomach. Liquid creatine is ineffective as a creatine supplement due to its limited stability in solution. This shouldn’t be an issue for people preparing a creatine solution at home, since it takes a few days to for creatine to degrade. This is a problem for the manufacturers, where creatine in solution has a limited shelf-life.
“Buffered” creatine (Kre-Alkylyn) is suggested to be a better absorbed form of creatine supplementation, but it can be rapidly neutralized in the stomach if it is not in an enteric coating. Even if it is enteric coated, there is no evidence to support its efficacy above creatine monohydrate.
Creatine ethyl ether is likely ineffective as a creatine supplement for general use.
Creatine magnesium chelate has some limited evidence for it being more effective than creatine monohydrate, but this has not been investigated further.
Other forms of creatine are equally ineffective, therefore stick to the proven and extremely affordable creatine monohydrate.
Loading Protocol:
- Take 5grams of creatine monohydrate 4-5 times per day for the first 5 days
- Continue with 3-5grams indefinitely, preferably before or after your workout or with a meal if it’s a non training day to avoid feeling nauseus.
This will ensure that you get all the benefits within a week of intake.
One of the most significant benefits of creatine supplementation is its ability to improve strength and power output during resistance exercise. Moreover, when combined with resistance training, creatine may slightly increase lean muscle mass. There have also been several studies investigating the effects of creatine on anaerobic running capacity, and while the findings are somewhat inconsistent, the general consensus is that creatine may lead to a minor improvement in performance.
While the research on the effects of creatine on cognitive performance is not as extensive as it is for physical performance. There is evidence to suggest that creatine supplementation may be beneficial in certain situations such as reducing mental fatigue in scenarios with demanding mental activity and sleep deprivation. It may also improve working memory, though likely only for people with below-average creatine levels, such as vegetarians and older adults.
Creatine supplementation enhances exercise performance, but most studies show that it has no effect on testosterone levels.
There is limited evidence on the link between creatine and DHT, and no studies have directly examined the effect of creatine on hair loss.
Limited short-term evidence indicates that people with suboptimal kidney function may safely supplement with creatine. However, long-term studies are lacking.
If you are someone with kidney dysfunction, or at risk for developing kidney dysfunction, you might wish to forgo creatine, or otherwise take only the lowest effective dose (3 g/day) Since creatine can increase water retention, it could theoretically harm people whose kidney disorder is being treated with diuretics, which cause water loss.
Cellular swelling, which occurs when creatine is absorbed and pulls water into cells, is associated with increased muscle cell growth.
A protective effect on neurons by creatine, secondary to its ability to donate phosphate groups, exists and appears to be quite general in its protective effects. Mitochondrial function appears to promote neuronal growth and proliferation, and at least _in vitro_, creatine is known to do the same and promote growth.
There appears to be a positive correlation between creatine and glycogen levels in muscle cells, such that an increase in one is often accompanied by an increase in the other. As a result, it is believed that creatine supplementation may contribute to glycogen replenishment and loading.
Taking creatine supplements along with carbohydrates can enhance the synthesis and accumulation of glycogen in skeletal muscles. However, while creatine supplementation can speed up glycogen replenishment rates, it does not seem to result in an increase in the amount of creatine that enters the cell.
Supplementing with creatine has been found to increase the size of muscle fibers, irrespective of protein synthesis. The lowest dose of creatine sufficient to increase muscular creatine stores in otherwise healthy but sedentary people (2 grams) appears to be insufficient for athletes. The benefits of creatine supplementation appear to be more prominent when taken closer to the resistance training workout than when compared to supplementation at other times of the day. This benefit applies equally to taking creatine before the workout and/or after the workout.
When exercising in heat, supplemental creatine (loading phase with carbohydrates) appears to be able to reduce symptoms of hyperthermia, such as perceived physical exertion. Despite physical performance enhancement only occurring in creatine responders, the benefits of heat tolerance occurred in both groups of people.
When examining repeated sprinting tests (sprint, rest a minute or less, repeat) the rate of phosphocreatine resynthesis appears to be a positive influence on performance and supplemental creatine appears to be beneficial.
Creatine supplementation does not appear to reduce the rate of muscle loss during immobilization, but appears to enhance muscular rehabilitation afterward.





